Reflections at the Georgetown University Medical Center Council of Chairs Meeting
Warwick Evans Conference Room – Building D
Georgetown University Medical Center
February 7, 2014
Good afternoon. I’m grateful for the invitation to join you today. It’s a privilege to have this opportunity to spend time together….to recognize the extraordinary contributions you and your departments make to our university…and to engage in a conversation about some of the pressing issues of the day.
I’d like to begin with some brief framing remarks that speak to the unique role the Medical Center plays in the mission of our university…then I’d like to offer some reflections on our current funding environment…and I’d like to close with some comments on a few issues that I know have been top of mind for many in this room. We’ll then leave plenty of time for questions on any topics you wish to discuss.
GUMC Mission
Gathered here today, we recognize the meaningful role that the Medical Center plays on our campus. You are engaged in a unique interplay of missions: teaching, research, and clinical practice – and with that comes a very complex set of issues, which you are constantly navigating, innovating in, and balancing.
Your contributions to our community enable us to maintain the highest standards of academic excellence, and we are committed to ensuring that the Medical Center will continue to play a critical role in addressing health challenges as well as biomedical research and education.
To put this in context, this is work that Georgetown has been committed to since the School of Medicine’s establishment in 1851. In the past 163 years, we’ve seen extraordinary changes to the field of academic medicine. We’ve navigated changing landscapes and adapted at each moment to ensure that our Medical Center’s mission is sustained and supported into the future.
So while this may be the most challenging environment of our generation, we’re still conducting superb research; educating superb students; and engaging in superb clinical practice.
Georgetown is classified by the Carnegie Foundation as a Research University with “very high research activity” (RU/VH) – the highest classification given to research universities and the equivalent of Tier 1 status – in large part because of the extraordinary research conducted by Medical Center scientists. We have more than 400 scientists on this campus working on basic and clinical research projects and more than 875 IRB-approved human research studies .
Roughly three-quarters of the research activity that takes place at Georgetown is happening on this Campus. And as I said at our Faculty Town Hall last week, this is all during the most challenging funding environment in our lifetime. We are grateful for the extraordinary contributions you and your colleagues make.
Additionally, because of your leadership and work, we are one of only 31 academic medical centers in the country to receive both a Clinical and Translational Science Award and the designation of a Comprehensive Cancer Center.
You also engage in the vital work of educating the next generation of doctors, researchers, and health workers.
The number of applications to the School of Medicine continues to be strong. This past year, we received 12,250 applications, giving 345 offers of acceptance and making our selectivity rate 2.8%—one of the best in the nation. The School of Medicine was also listed on the US News and World Report’s “Short List” for the 10 most selective schools in the country, and our graduating medical students routinely match at some of our nation’s top clinical programs.
The Medical Center also continues to be a source of innovative biomedical graduate educational programs, including the online Nursing at Georgetown program, three NIH-funded training grants that provide 32 doctoral and postdoctoral stipends each year, and a growth in interdisciplinary masters of science programs that have a current enrollment of over 470 students.
We are also, as you know, engaged in a university-wide capital campaign, For Generations to Come: The Campaign for Georgetown. The Campaign represents a significant effort by our community to provide student financial aid at the undergraduate and graduate levels, as well as investments in faculty research, infrastructure, and in transformative opportunities – ideas that will generate the kind of innovations in scholarship and teaching that will impact our community for generations.
As part of our “Transformational Opportunities” campaign pillar, we’re engaging new ideas in biomedical research and health care education; personalized cancer treatment; research on neurological diseases; and developments in global health, among many others.
We’re grateful for the work that you and your faculty do, for your commitment to Georgetown, and for the ways that we’re able to come together to continue our efforts to become a better and stronger institution.
Research Reflections
Now, as I said a few minutes ago, we are confronting the most challenging funding environment for research in our lifetime. At last week’s Faculty Town Hall, I offered some reflections on the context in which we find ourselves and to which we are working to adapt.
Current Funding Environment
One of the ways we can assess the context for university research is to look at the funding environment. Since World War II, the crucial driver of the research missions of our universities has been Federal investment through the NIH, DOD and NSF.
Chart 1: Federal Investment in Research since 1976
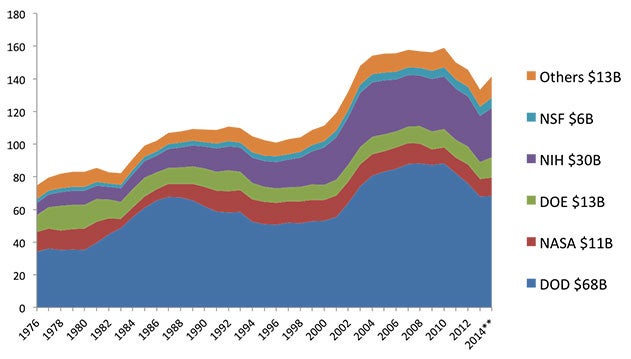
Chart 1, which draws on data from the NSF, will give you a sense of the Federal investment in research since 1976.
Chart 2: University R&D Spending by Funding Source ($ in billions)
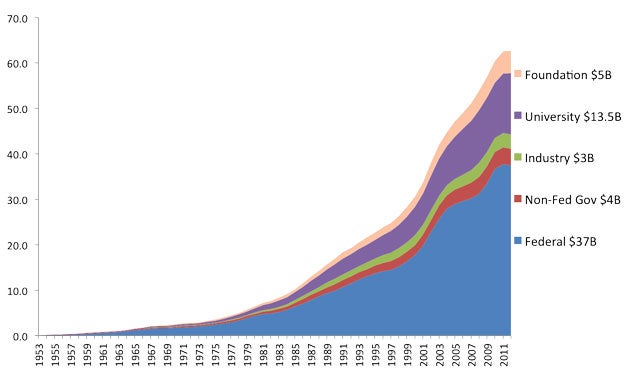
Chart 2, also drawing on data from the NSF, will give you another perspective on the place of the Federal government in supporting university research.
Chart 3: The role of the Federal government in supporting university research II
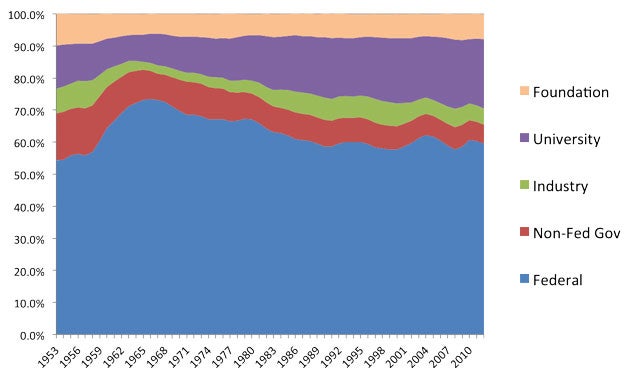
Chart 3, similarly drawn from NSF data, presents another way of showing the sources of support for university research.
I think this slide demonstrates a very powerful dynamic that has evolved over the past generation—the increasing responsibility of universities to fund research.
In 2012, the Federal government provided $37.4 billion in support of research to universities (Research & Development). The same year, universities spent $13.7 billion of their own resources (NSF). The ratio of university to federal spending is 36%. For most of the period following World War II that number was closer to 20%.
For Georgetown, the most significant extramural support has come from the NIH and DOD for life science research. As a university, we conduct $180 million worth of research. Roughly three-quarters of our research takes place at our Medical Center.
This is the most challenging funding environment in our lifetime.
Chart 4: NIH Funding Trend ($ in billions) (History of Congressional Appropriations)
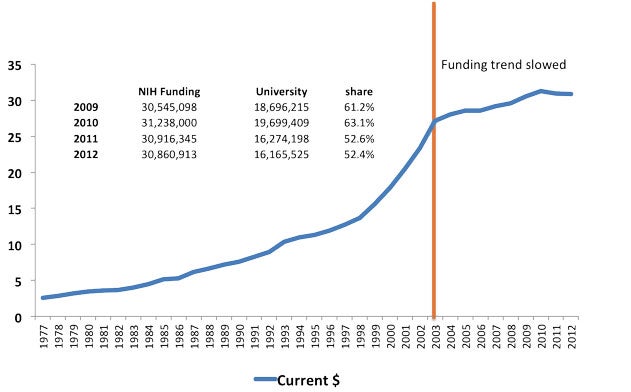
The “sequester” weakened an already deteriorating commitment of support for research in our nation. As a result of sequestration, support for research at the National Institutes of Health has declined 5.5% (Rockey and Collins); overall Federal support for research has declined 3.3% (NSF). The amount of spending on research at our nation’s universities declined this past year for the first time since 1974 (NSF).
As a result of the decline in investment, at the NIH, only 1 in 6 proposals reviewed can be funded—the lowest rate in our lifetimes (NIH Fact sheet).
Chart 5: NIH Grant Application Success Rates (Rockey and Collins)
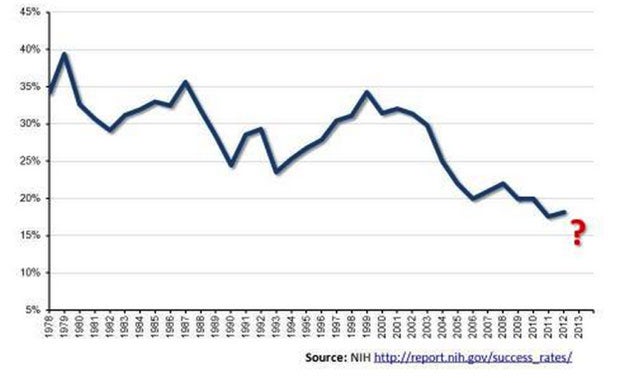
We received very good news on January 17 when President Obama signed the 2014 federal budget into law. The new budget increases NIH funding by $1 billion (Committee on Appropriations). But even with this increase, funding for the NIH will still be below the 2012 level of funding. This increase restores $1 billion of the $1.55 billion cut as a result of the sequester (NIH Fact sheet).
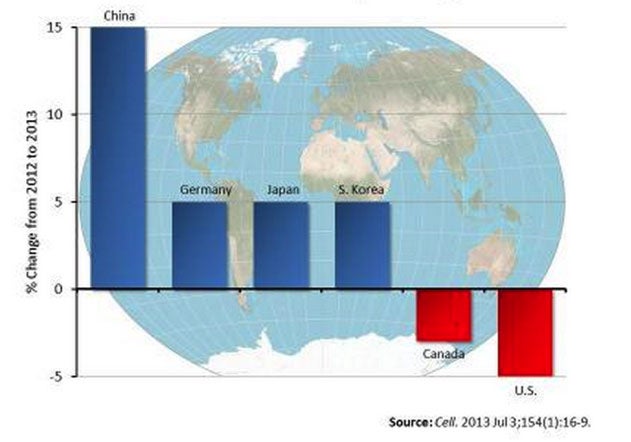
This is occurring at time when other countries are significantly increasing their commitment to research. China has increased spending by 15% (Rockey and Collins). Between 1999 and 2009, the U.S. investment in research and development dropped from 38 to 31 percent of the world total; Asian nations’ share increased from 24 to 32 percent (“NIH Turning Discovery Into Health”).
Chart 6: Global Scientific R&D Spending (Rockey and Collins)
The model that has shaped our nation’s research efforts for seventy-years is changing and we will have to adapt to these changes.
Research
It is within this funding environment that we recognize we must find new ways to fill the gap left by decreased government funding to ensure that we maintain and enhance a strong research trajectory. As a university, we remain as committed as ever to investing in creating the context for continued excellence and growth in research. MedStar is essential to this.
As a university, we have invested $100 million in the Medical Center over the past five years, which is only a portion of what is required to make us a leading academic clinical enterprise. MedStar’s contribution of $36.7 million in gain-sharing over that period has been essential to maintaining our academic medical mission in the short term; however, we must continue to work together toward creating a stronger, predictable, sustainable financial model for the future.
We strongly believe that the best strategy for our partnership with MedStar is to pursue collaborative, strategic long-term planning for all the ways we work together – including both support for the research enterprise and the use and improvement of our clinical facilities.
Infrastructure
With respect to the physical plant, I know there are significant facilities issues and constraints at the Medical Center and the Hospital, and wish to be as supportive as possible of any MedStar effort to upgrade or renovate MedStar Georgetown University Hospital.
To that end, the University has over the last year devoted significant resources – very meaningful amounts of time, money and energy – to establishing a framework to grow and develop. This framework is built on the fundamental principle of engaging in a purposeful, on-going, collaborative partnership with key stakeholders – including the city and the surrounding neighborhoods – to pursue long-term planning that will satisfy the goals of all parties.
We believe the framework we have developed holds great promise for the University and for our clinical partner, MedStar Health.
The University is already seeing the rewards of this approach. Our relationship with the city and the community has never been better, and the use of this framework of collaborative partnership and planning has allowed us to grow enrollment, to begin new construction projects, and, most importantly, to plot a path for the University’s future growth and development.
We believe this framework creates a path for MedStar’s re-development of the hospital as well, and have engaged MedStar in a collaborative planning process to advance its plans for the future use of its footprint, including a new or renovated Georgetown University Hospital.
We have specifically worked with them to develop an approach for integrating the needs of the clinical enterprise into the required long-term planning for the footprint and have made considerable progress towards developing a plan that meets both of our needs.
We look forward to continuing our work with MedStar, and I expect our colleagues from MedStar will be sharing with you more specific plans for the improvement to the physical plant and facilities, which I know are essential to the academic medical mission.
Joint Philanthropy
We are also engaging with MedStar to develop a joint-philanthropic framework. Philanthropic support has always been critical to medical research and teaching, and it will only become more so as federal and other external sources of funding continue to be constrained. By developing a joint-philanthropic structure with MedStar, we believe our shared enterprise will be best positioned to build a stronger and broader base of donors and prospective donors to best support the mission of the Medical Center.
Closing
Thank you for you time today. Again, I’m grateful for all that you do. Your contributions – whether through clinical practice, research, or medical education – are essential to our mission as a university.
It is because of your leadership and work…along with our collaborative, long-term and strategic planning with MedStar– guided by the principles we’ve established – that we believe we will achieve the joint development of this campus; a stronger research trajectory; and a more predictable, sustainable business model that will allow us to continue and strengthen the Medical Center mission.
Works Cited
Britt, Ronda. “Higher Education R&D Expenditures Remain Flat in FY2012.” Info Brief – National Center for Science and Engineering Statistics. National Science Foundation. Nov. 2013. Web.
“Fact sheet: Impact of Sequestration on the National Institutes of Health.” National Institutes of Health. 30 Jan. 2014. Web.
Grueber, Martin and Tim Studt. “2012 Global R & D Funding Forecast: Stable Growth of U.S. R & D.” Research & Development. 30 Jan. 2014. Web.
“History of Congressional Appropriations.” NIH — Office of Budget —Appropriations History by Institute/Center (1938 to Present). National Institutes of Health, n.d. Web. 30 Jan. 2014.
“NIH Turning Discovery Into Health: Global Competitiveness – The Importance of U.S. Leadership in Science and Innovation For the Future of Our Economy and Our Health.” National Institutes of Health. Web.
Rockey, Sally, and Francis Collins. “One Nation In Support of Biomedical Research.” NIH Extramural Nexus. NIH, 24 Sept. 2013. Web. 30 Jan. 2014.
“Summary: Fiscal Year 2014 Omnibus Appropriations Bill.” Committee on Appropriations. 13 Jan. 2014. Web.